The primary goal of periodontal therapy is the reduction or elimination of inflammation. Traditionally, this is accomplished through removal of subgingival tooth‐borne accretions using non‐surgical and/or surgical treatment modalities. Numerous studies indicate the difficulty in removing these accretions. Studies show when treating 4->6mm probing depths with scaling and root planning alone, only 30-40% of the root surface is plaque free.
Typically the type of healing response after scaling and root planning is a type of repair ( long junctional epithelium) adhesion to the root surface. Our primary goal should be, regeneration of the original connective tissue fiber attachment to the root surface along with periodontal ligament and bone.
Traditionally treatment of moderate to advanced periodontal disease begins with, Phase I, scaling and root planning. Several weeks later a re-exam assesses the results of Phase I. Sites that still show probing are then treated with surgical therapy.
Over the past few years I have been combining two different technologies to overcome the limitation of traditional scaling and root planning and to limit the possibility of periodontal surgery,
- Perioscopy- I have been using the Perioscope to achieve a dramatic increase in plaque and calculus free root surfaces. This endoscope has a small camera which is placed in the periodontal pocket and on a TV monitor I can readily see the acretions on the root at 48x magnification. This technology maximizes the body’s healing response. I routinely see very deep probing depths reduce to a normal sulcus.
- Laser therapy- I have been using laser therapy for several years. Lasers have numerous tissue interactions such as ablation or vaporization, hemostasis, microbial inhibition and destruction , as well as biological effects, such as biostimulation (photo-bio-modulation), which induce various beneficial therapeutic effects and biological responses. Research has shown that regeneration of periodontal ligament and bone is possible with this modality.
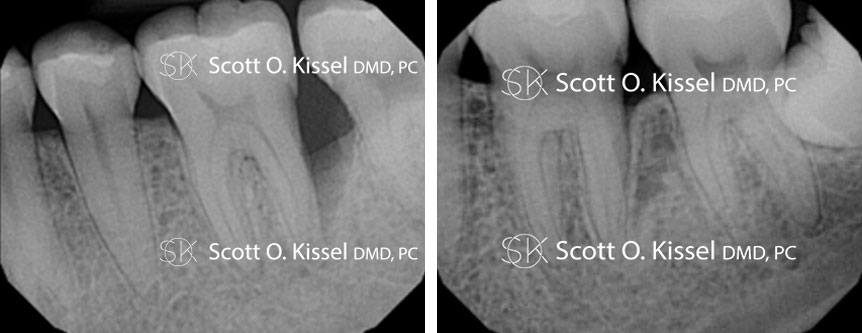
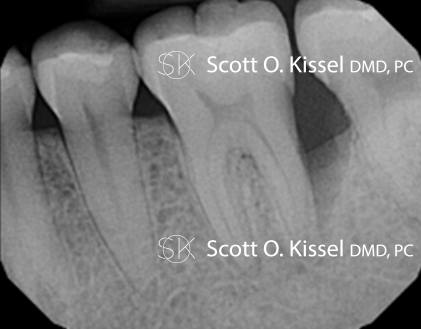
Below are radiographs of a patient who presented with generalized moderate to advanced periodontal disease. Tooth #19 shows a deep distal periodontal pocket of 9mm and bleeding upon probing. She was treated with the Perioscope and laser therapy. The one year post op film shows complete resolution of the bone defect. Even lamina dura is present (compact bone that lies adjacent to the periodontal ligament, in the tooth socket), which when evident signifies the presence of true bone and pdl. If you look closely, you can see the border of the previous bone defect and the regenerated structures.
Using this approach I am routinely seeing regeneration of tissues. In my practice, the frequency of using microsurgery to treat periodontal disease, has been significantly reduced. Like you, I now have cabinets full of infrequently used materials that will grow old as the practice evolves. If you have any patients that are looking for a non-surgical regenerative alternative to treat even advanced periodontal disease, this is the option I recommend.