
Gum Disease vs. Gingivitis: Understanding the Stages
Confused about gum disease and gingivitis? NYC periodontist Dr Kissel explains the stages, treatment options, and the importance of early intervention.
Confused about gum disease and gingivitis? NYC periodontist Dr Kissel explains the stages, treatment options, and the importance of early intervention.

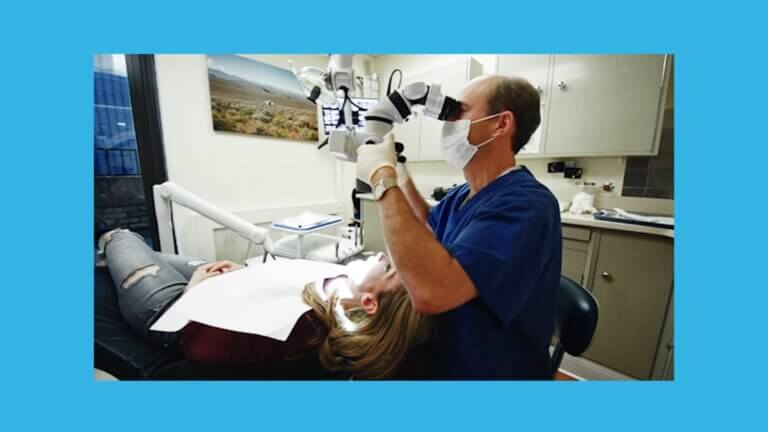
Discover the effectiveness of dental microsurgery for precise and minimally invasive gum disease treatment. Contact Dr. Scott Kissel for personalized care in Midtown Manhattan, NYC.

Learn how dental microsurgery can improve crown lengthening results and offer a less invasive, more comfortable experience, with Manhattan periodontist Dr. Kissel.

Experience the transformative power of SMILE Technique dental Implants, a revolutionary technique that restores your smile in a single visit, providing natural-looking results and a boost in confidence.
Learn how to spot the symptoms of gum disease before it’s too late and how Dr Kissel, a top periodontist in New York, can help you.
Which types of dental implants are right for you? Learn about the different types and how Dr Kissel can help you restore your smile.

Dental microsurgery is a revolutionary technique that uses a dental microscope and fiber optic lighting system to perform dental procedures with more precision, accuracy, and
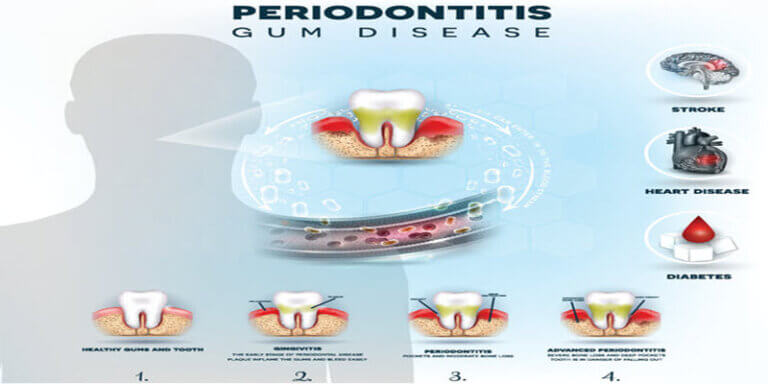
Periodontitis, a common dental condition, can have a significant impact on oral health if not properly managed. According to Dr. Kissel, periodontitis is a stage
Dental implants have become one of the most popular tooth replacement options but as many people know, the dental implant procedure can take months to